Section : Neuroradiology
Case Type : Clinical Cases
Authors : Rashmi Kotkar, Madhuri Ghate, Geetanjalee Kadam, Amol Gulhane, Shriyesh Jaiswal, Shubham Kabra Krsna Diagnostics PVT LTD; Pawana Nagar Housing Society 411033 Chinchwad, India; Email:madhuri.ghate01@gmail.com
Patient : 20 years, male
Categories :
Area of Interest : Neuroradiology brain
Imaging Technique : MR-Angiography
Procedure : Education
Special Focus : Trauma
CLINICAL HISTORY :
A 20-year-old male patient presented with a headache and a scalp swelling in the left frontal region. He had a road traffic accident 3 months back. A plain CT brain examination performed at that time was within normal limits. He was referred to the neurosurgeon who advised MRI brain examination with MR angiography.
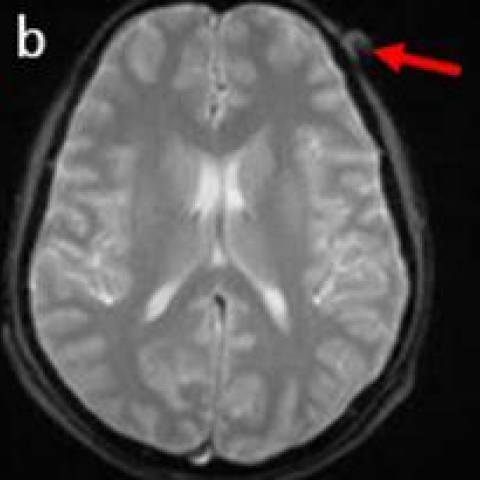
IMAGING FINDINGS :
The MRI brain examination of the patient was within normal limits except for a small well-defined oval lesion in the subcutaneous plane in the left frontal region. It was isointense on T1 with a small hyperintense dot within and patchy blooming within on GRE – suggestive of thrombus. It appeared heterogeneously hyperintense on T2WI. (Fig. 1 a, b, c). An MR angiography (MRA) (TOF) of the intracranial vessels was within normal limits. When external carotid artery was traced, the frontal branch of the Superficial Temporal Artery (STA) was seen coursing up to the base of the lesion in the scalp in left frontal region measuring 1.1 x 0.8 cm in size, which was suggestive of a thrombosed pseudoaneurysm (Fig. 2, 3 and 4).
DISCUSSION :
Aneurysms are classified as true and pseudoaneurysm. A majority of cases are true whilst pseudoaneurysms represent less than 1% of cases [1]. Dilatation of the intact arterial wall results in true aneurysms while a total or partial rupture of the arterial wall, generally secondary to trauma, results in pseudoaneurysms which will further complicate into haematoma formation and organisation [2, 3]. The most common aetiology resulting in pseudoaneurysms is blunt trauma from sports-related injuries, motor vehicle accidents and missile injuries. Penetrating injuries from stab wounds, gunshots, lacerations and surgery can also cause pseudoaneurysms [4, 5]. Pseudoaneurysm of the STA commonly affects more men than women, however, a few paediatric cases have also been reported [6, 7]. The STA is the terminal branch of the external carotid and has an anterior or frontal branch and a posterior or parietal branch. It is vulnerable to trauma and aneurysm formation due to its superficial location directly against the skull between the frontalis and temporalis muscles [8]. The STA pseudoaneurysm can be primarily diagnosed on history and physical examination. Patients usually have a history of trauma before development of the mass, which can be presented in acute (within 2-4 days) as well as in delayed phase (2-4 weeks), as in this case. On examination, the mass is pulsatile, and a bruit can be auscultated over the mass. With proximal compression of the STA, the pulsations can diminish or the mass can disappear. DSA and arteriography are gold standard investigations. However, ultrasound Doppler or CT angiography (CTA) or MRA should be advised as initial investigations for diagnosis. In cases of thrombosed aneurysm ultrasound is less specific. Plain CT brain examination can be reported normal as in this case. MRI brain examination with MRA is more useful in cases of delayed presenting aneurysms as intraparenchymal abnormalities, can also be better assessed and with postprocessing such as MIP reconstructions, information such as feeding branch vessel, status of thrombosis, size of aneurysm and other relevant information for surgery can be given. The standard treatment has been excision and ligation of the proximal and distal ends of the STA. Other treatment options are embolisation or ultrasound-guided percutaneous thrombin injection. However, non-target embolisation and autolysis of the embolisation material over time are possible complications [9]. Pseudoaneurysm should always be suspected in a trauma patient with a pulsatile swelling and appropriate investigation should be performed with CTA or MRA for its diagnosis to avoid devastating complications such as rupture.
DIFFERENTIAL DIAGNOSIS LIST :
Traumatic thrombosed pseudoaneurysm of Superficial Temporal Artery (STA).
Haematoma
Sebaceous cyst
FINAL DIAGNOSIS :
Traumatic thrombosed pseudoaneurysm of Superficial Temporal Artery (STA).