Clinical History:
A 24-year-old woman presented with a slow-growing swelling on the left side of her neck present for 6 months
Imaging Findings:
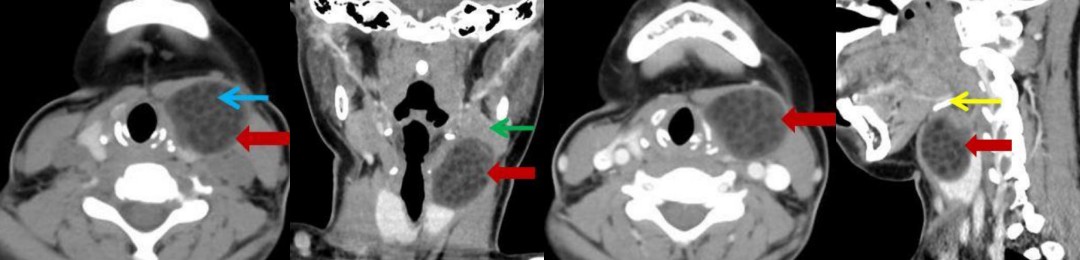
Axial pre- (Fig. 1) and post-contrast (Fig. 2) CT of the neck was performed with coronal (Fig. 3) and sagittal (Fig. 4) reconstructions. This showed a well-defined, thin-walled, subtly enhancing unilocular hypodense lesion (red arrow), containing multiple small fat density globules (blue arrow), with a characteristic ‘sac of marbles’ appearance. The lesion was located in the infrahyoid neck (hyoid bone-yellow arrow), in the left paratracheal region. It measured approximately 42 x 32 x 28mm (CC x Trans x AP) in size. The lesion lay superolateral to the left lobe of the thyroid gland, causing mild compression and indenting the posterior border of the left submandibular gland (green arrow). It was positioned inferior to the left mylohyoid muscle and did not reach the skin. No evidence of calcification was seen.
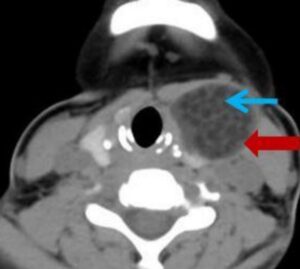
Figure-1
Description: : Axial non-contrast image of neck showing a well defined hypodense lesion(red arrow) in the left paratracheal region containing multiple fat density globules (blue arrow) giving the characteristic ‘sack of marbles’ appearance.
Origin: © Krsnaa Diagnostics Pvt Ltd, Chinchwad, Pune
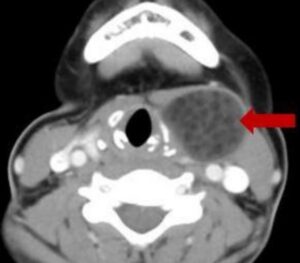
Figure-2
Description: Axial post-contrast image of the neck showing subtle peripheral enhancement (red arrow).
Origin: © Krsnaa Diagnostics Pvt Ltd, Chinchwad, Pune
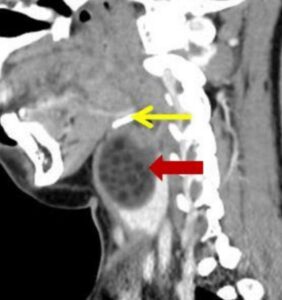
Figure-3
Description: Sagittal reformatted image showing the infrahyoid location (Hyoid bone -yellow arrow) of
the dermoid cyst (red arrow)
Origin: © Krsnaa Diagnostics Pvt Ltd, Chinchwad, Pune

Figure-4
Description: Coronal reformatted image showing the dermoid cyst (red arrow) abutting the left
submandibular gland (green arrow).
Origin: © Krsnaa Diagnostics Pvt Ltd, Chinchwad, Pune
Discussion:
The term dermoid cyst encompasses true dermoid cyst, epidermoid cyst, and teratoma, which are closely related histologically. Dermoid and epidermoid cysts are believed to be types of inclusion cysts whereas teratomas are considered neoplastic, containing all three germ layer elements [1].
Dermoid cysts are lined by squamous epithelium (derived from ectoderm) and contain dermal derived elements like skin appendages, hair follicles, sebaceous and sweat glands. Epidermoid cysts contain desquamated epithelium and keratin, and cholesterol debris. Dermoids can be differentiated from epidermoids as the latter do not contain dermal elements [2].
Dermoid cysts occur primarily in sites where embryonic parts fuse together. The majority of cases have been reported in the midline of the body and also in ovaries and testes. A paramedian location is less common. Approximately 7% of cases are found in the head and neck region [3]. The lateral eyebrow is the most common location [4]; the oral cavity being the second most common.
They usually present in the second and third decade [2] with equal sex distribution. In the neck, they present as a slow-growing swelling in the midline in the submental or submandibular space or rarely off-midline [5, 6]. Typically, the mass is mobile, soft and not attached to overlying skin.
On ultrasound a dermoid cyst appears as a well-circumscribed, unilocular hypoechoic cyst that may contain homogeneous internal echoes or multiple echogenic fat globules.
On CT typically the dermoid cyst appears as a well-defined peripherally enhancing thin-walled unilocular hypodense cystic lesion. Multiple small fat-attenuation globules are seen within it giving it a characteristic “sac of marbles” appearance, which is pathognomonic of the condition [7]. They may have a heterogeneous imaging appearance due to the presence of different germ layer components.
On MRI they can be hyper- to iso-intense on T1WI and hyperintense on T2WI. Fat is suppressed on STIR images. They have a heterogeneous appearance that differentiates them from epidermoid cysts and ranulas which usually have homogeneous fluid signal. Multiplanar imaging modalities are recommended to visualise the relation of the lesion to the mylohyoid muscle to guide surgical management. If the lesion is located superior to mylohyoid it is removed by an intra-oral approach. Lesions inferior to mylohyoid are removed by an external approach [8].
Our case was managed surgically with an external approach.
Differential Diagnosis List:
Dermoid cyst of the neck., Lipoma, Epidermoid cys
Final Diagnosis:
Dermoid cyst of the neck.
References:
Smirniotopoulos JG1, Chiechi MV (1995) Teratomas, dermoids, and epidermoids of the head and neck. Radiographics 15(6):1437-55 (PMID: 8577967)
Mahesh Kumar Mittal, Amita Malik, Binit Sureka, Brij Bhushan Thukral (2012) Cystic masses of neck: A pictorial review. Indian J Radiol Imaging 22(4): 334–343 (PMID: 23833426)
Koeller KK, Alamo L, Adair CF, Smirniotopoulos JG (1999) Congenital cystic masses of the neck: radiologic-pathologic correlation. Radiographics 19(1):121-46 (PMID: 9925396)
New G (1947) Congenital cysts of the tongue, the floor of the mouth, the pharynx, and the larynx. Arch Otolaryngol 45:145-158 (PMID: 20290271)
Som PM, Sacher M, Lanzieri CF, Solodnik P, Cohen BA, Reede DL, Bergeron RT, Biller HF. (1985) Parenchymal cysts of the lower neck. Radiology 157(2):399-406 (PMID: 4048447)
Howell CJ (1985) The sublingual dermoid cyst. Report of five cases and review of the literature. Oral Surg Oral Med Oral Pathol 59(6):578-80 (PMID: 3859819)
Hunter TB, Paplanus SH, Chernin MM, Coulthard SW (1983) Dermoid cyst of the floor of the mouth: CT appearance. AJR Am J Roentgenol 141(6):1239-40 (PMID: 6606323)
Vogl TJ, Steger W, Ihrler S, Ferrera P, Grevers G (1993) Cystic masses in the floor of the mouth: value of MR imaging in planning surgery. AJR Am J Roentgenol 161(1):183-6 (PMID: 8517299)